June 1, 2022
Using MBC to treat TRD in practice today

Written by
L. Alison McInnes, MD, MS




A large body of research has shown that measurement-based care (MBC) can improve clinical outcomes and provide a number of benefits to both providers and patients in mental health care.
Among its benefits, MBC can:
- Improve patient outcomes and significantly increase the therapeutic effect size
- Detect symptom deterioration and acute situations faster
- Increase therapeutic efficiency, resulting in faster symptomatic improvement
- Increase patient adherence to medication and treatment protocols
As a result, patients feel more engaged and informed. They're also more in tune with their own progress and can recognize early signs of relapse or promising signs of improvement. Finally, patients find that this approach democratizes the relationship with the provider and enhances overall communication.
Even with clear benefits to MBC, the vast majority of Psychiatrists don't implement it.
In this 3-part series, we'll cover:
•Why MBC is key to unlocking better patient outcomes
•Barriers to implementing MBC
•The best ways to implement MBC that don't take a ton of extra time.
First, let's cover what MBC is, and guiding principles.
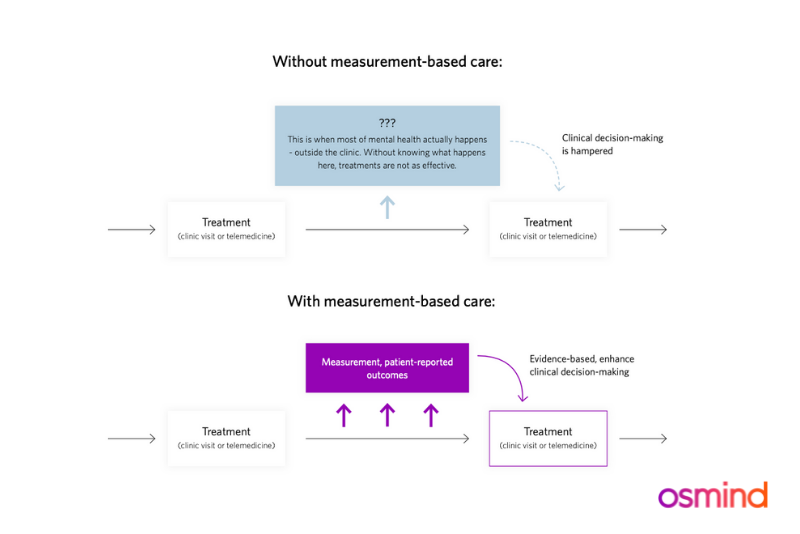
What is measurement-based care?
Measurement-based care (MBC) is an evidence-based practice that refers to the systematic evaluation of patient progress throughout a treatment, including systematic administration of symptom rating scales, which helps drive clinical decision-making in a personalized manner. Evidence has shown that MBC improves clinical outcomes, therapeutic efficiency, and patient adherence. In 2020, Osmind published a white paper on MBC, highlighting its many benefits for both clinicians and patients, and how it can improve clinical outcomes for the latter.
As a result, patients feel more engaged and informed. They are also more in tune with their own progress and can recognize early signs of relapse or promising signs of improvement. Finally, patients find that this approach democratizes the relationship with the provider and enhances overall communication.
MBC also provides crucial real-world data about the efficacy of treatments beyond the evidence generated in clinical trials. In January 2021, Osmind, in collaboration with physician-scientists at Stanford University School of Medicine, published the largest real-world data study on ketamine infusion therapy in the Journal of Affective Disorders. The analysis found that ketamine was a rapid, effective, and durable treatment for depression and that over 70% of patients with suicidal ideation at baseline experienced an overall improvement. Real-world evidence (RWE) like this is critical for increasing accessibility to innovative mental health treatments for patients who need it most.
Accurately measuring health outcomes in mental health is not as straightforward as in other medical specialties. However, this does not mean there is nothing that clinicians can do to improve the accuracy of mental health tracking. Below are three ways you can implement MBC into your practice:
1. Measure the good
Measurement-based care (MBC) involves the routine administration of validated outcomes measures to patients and discussion of that data with the patient. As we currently have no objective biological measures to let us know whether or not a treatment has succeeded, it’s imperative that we be able to reference outcomes data to justify maintaining or changing a particular course of therapy. Additionally, we clinicians that care for patients with treatment-resistant depression (TRD) have a heightened responsibility to help manage expectations about new treatments for our patients who may be suicidal and/or incur financial hardship to receive care.
How will we know the treatment is working? This is a critical question to answer with the patient before starting on a relatively novel treatment like ketamine. I argue that the question is best addressed with baseline and repeated mood assessments in order to methodically track target symptoms. I also find that with ketamine therapy, certain symptoms, like increased energy and initiative, will improve before mood per se and systematically querying all the symptoms in a depression survey can help illuminate promising changes.
I involve patients in their care journey by using the Osmind patient app. The app asks patients to track how they’re doing between visits, using mood scores and/or other validated survey questionnaires. Patients receive notifications and text messages to remind them to complete these measures, which allow both clinician and patient to more effectively track progress together. The goal is to help patients become more engaged in their care, which can give them more control and agency as the primary stakeholder of their own health.
2. Do no harm
Not everyone responds to ketamine therapy and we need to be on the alert for clinical deterioration during the treatment. Aust et al. 2019 showed that some patients have an anxious dysphoric response induced by ketamine and these patients are not likely to be responders. Hatfield et al. 2010 point out that therapists are not good at detecting clinical decline in patients in the absence of systematic symptom assessments.
Furthermore, only 18% of psychiatrists and 11% of psychologists routinely practice MBC, according to a collaborative report from the Kennedy Forum among others. We need to do better. The Osmind EHR was built with MBC at its core and allows clinicians to receive insight into treatment progress and detect symptom deterioration if it occurs.
3. Protect the clinician-patient relationship
Outcomes data are mandated as part of the Spravato/esketamine Risk Evaluation and Mitigation Strategy (REMS) program and every psychedelic drug that eventually meets FDA approval will also be associated with a mandatory REMS program.
REMS programs are put in place to ensure uniform practice standards and protect patients from adverse events. These programs also provide med-legal protection for clinicians as appropriate documentation is the best defense in the case of an adverse event.
At Osmind, we want to protect and serve our clinicians by making this documentation fast and easy. The Osmind ketamine EHR is the only one on the market offering Spravato/REMs automated submission and we will be developing similar modules for new psychedelic medicines as they come to market.
As clinicians who have dedicated our lives to improving the lives of patients with mental health conditions, we should embrace outcomes assessments. Measurement-based care is the practice of evidence-generating medicine and the real-world data we gather from routine patient visits will shape the future of mental health treatments.
Now you have the foundations of why measurement-based care (MBC) matters. In part 2, we'll cover why patients drop out of therapy, and how to engage and retain them throughout the process.
About Dr. Alison McInnes
Dr. Alison McInnes is Vice President, Medical Affairs at Osmind. She is a nationally recognized expert in psychiatry and mood and anxiety disorders, having specialized in treating refractory disease for over a decade. She is an expert in ketamine treatment and psychedelic medicine. McInnes founded and served as Medical Director for Kaiser Permanente's ketamine infusion therapy program for a number of years, and was previously an Associate Professor of Psychiatry at Mount Sinai School of Medicine for 8 years where she ran a lab in psychiatric genetics. She was also an adjunct clinical professor at UCSF.
Dr. McInnes is regularly invited to speak at national and international conferences and consults for biopharmaceutical companies working at the cutting edge of neuropsychiatry. She is a member of the American Society of Ketamine Physicians, Psychotherapists and Practitioners (ASKP3) Certification Governance Commission, which is an autonomous governing body that oversees the development, implementation, and management of a certification program for clinicians offering ketamine therapy. In her current clinical practice, she focuses on treatment-resistant mood disorders and complex cases.
Dr. McInnes received Bachelor’s and Master’s degrees from Stanford University and her MD from Columbia University. She completed her residency at UCSF and research at the VA Research Fellowship and Howard Hughes Physician Research Fellowship in Psychiatric Genetics at UCSF.
Connect with forward-thinking peers, advance your practice, and attend expert events. Join the Psychiatry Collective today.
.png)
.png)
If you, or someone you know, is in crisis or needs immediate assistance, please call 911 immediately. To talk to someone now, please call the National Suicide Prevention Lifeline at 1-800-273-8255 or 988.
Osmind © 2026 All Rights Reserved.

.png)
.png)