June 20, 2022
Boosting ketamine therapy patient retention

Written by
Dr. Alison McInnes




This is the second in a series of articles from Dr. McInnes on how clinicians can implement measurement-based care into their daily practice. The first article, “How to use measurement-based care to achieve better outcomes for patients with treatment-resistant depression,” can be read here.
What is patient retention?
Patient retention is defined as the percentage of patients who return to complete a course of treatment after an initial visit, or for our purposes, those who complete a ketamine induction. It’s also an important metric for measuring the success of medical practices. There is a strong body of evidence that measurement-based care (MBC) improves patient retention and engagement in treatment.
Pragmatic preparation and integration using measurement-based care
At Osmind, we are also turning MBC data into real-world evidence that supports breakthrough mental health treatments. Earlier this year, we published the largest real-world data study on ketamine infusion therapy (KIT) in the Journal of Affective Disorders in collaboration with physician-scientists at Stanford University School of Medicine. The first analysis of Osmind Real-World Ketamine Analyses (ORKA), ORKA-1, found that ketamine was a rapid, effective, and durable treatment for depression and that over 70% of patients with suicidal ideation at baseline experienced an overall improvement. Since then, we have continued to analyze depression and anxiety outcomes data in our second dataset (ORKA-2) of real-world patients receiving KIT induction, and several findings have emerged with striking implications for the daily practice for mental health clinicians.
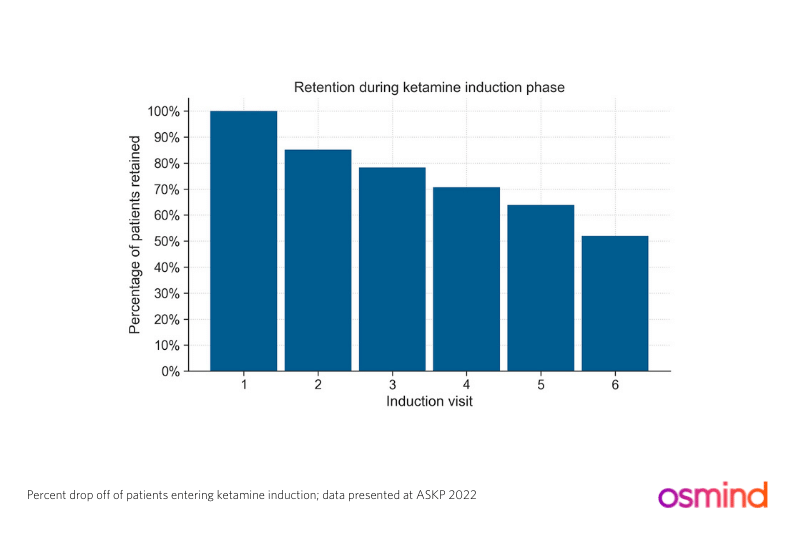
While reviewing data from a new sample of 10 affiliated ketamine practices gathered between 2017 and 2020, I was interested to note that almost 50% of patients did not complete all 6 infusions and 20% of patients dropped out after the first infusion [data for ORKA-2 presented at ASKP3 2022, the fifth annual conference of the American Society of Ketamine Physicians, Psychotherapists, and Practitioners].
Why do so many patients drop out after the first ketamine infusion?
Patients may leave treatment for many reasons, chief among them that it imposes a significant financial burden. Factoring in cost, I could see patients leaving early because they do well and don’t want to continue to pay, but I tend to think it’s non-response to the first few infusions that is likely the culprit. Looking at the data from our first paper, ORKA-1, we see that less than 30% of the patients responded to the first infusion (table 1). Our thinking about how to maximize the chance for response has changed significantly since the earliest days of ketamine therapy and the literature now supports continuing induction infusions until response is achieved or a total of 6 infusions have been administered.
Specifically, two studies of repeat infusions (6) within 2-4 weeks demonstrated that some patients may not respond to the first infusion(s) and may instead convert to responder status later in the induction protocol (Philips et al. 2019) especially if they are older (Pennybacker et al 2021). Our supplementary data from ORKA-1 also shows that response rates increase with each infusion up to 6.
Patients leaving before trying 6 infusions are missing an opportunity to benefit, although if they attain response earlier we still have no data to suggest that continuing induction infusions further improves outcomes (i.e. a chance for remission or longer duration of antidepressant response) – this is certainly an interesting area for further research. We also know from the ORKA-2 data set that maximum response is achieved after the induction is complete such that additional infusions may help maintain response but they are not going to improve it, at least in this data set. In other words, non-responders after induction (most commonly 6 infusions) are unlikely to respond if infusions are continued.
So what can clinicians do to aid retention?
- Have a discussion with patients on symptoms while you are reviewing data from their baseline mood surveys with them. Patients may not have a thorough understanding of how and when symptom improvement could be expected and measured. I believe this process is an essential part of the preparation phase for ketamine therapy whether it be KIT or ketamine-assisted psychotherapy (KAP).
- Share the data on ketamine response above that suggests the best chance for success is to keep going with infusions till response is achieved, or to infusion 6 – whichever comes first.
- Give patients an opportunity for integration the day after the session. This can help them process their disappointment if they experienced unwanted side-effects and/or no immediate change in mood.
- Let patients know that the effects of ketamine therapy are likely to wane and that they should feel welcome to return if this happens for them. This could happen if patients do respond and don’t want to keep paying for expensive treatments. ORKA-1 found that there was an 80% chance of retaining a response at one month and 60% at two months; however this is just one study and we need more data to know for sure how long the antidepressant effects of an induction last.
Our goal at Osmind is to help patients become more engaged in their care, which can give them more control and agency as the primary stakeholder of their own health. The authors of one review article that examined over 50 studies wrote, “Virtually all randomized controlled trials with frequent and timely feedback of patient-reported symptoms to the provider during the medication management and psychotherapy encounters significantly improved outcomes.”
As a clinician myself, I’m a big proponent of mood surveys and collaborative care, and believe the impact of MBC on patient engagement and retention cannot be understated.
Now you know why patients drop out of Ketamine treatment, and ways to retain them. In part 3 of the MBC series, we'll dive into how you can use MBC to empower your patients get the most out of Ketamine infusions and Ketamine-Assisted therapy (KAT).
About Dr. L. Alison McInnes
Dr. L. Alison McInnes is Vice President, Medical Affairs at Osmind. She is a nationally recognized expert in psychiatry and mood and anxiety disorders, having specialized in treating refractory disease for over a decade. She is an expert in ketamine treatment and psychedelic medicine. McInnes founded and served as Medical Director for Kaiser Permanente's ketamine infusion therapy program for a number of years, and was previously an Associate Professor of Psychiatry at Mount Sinai School of Medicine for 8 years where she ran a lab in psychiatric genetics. She was also an adjunct clinical professor at UCSF.
Dr. McInnes is regularly invited to speak at national and international conferences and consults for biopharmaceutical companies working at the cutting edge of neuropsychiatry. She is a member of the American Society of Ketamine Physicians, Psychotherapists and Practitioners (ASKP3) Certification Governance Commission, which is an autonomous governing body that oversees the development, implementation, and management of a certification program for clinicians offering ketamine therapy. In her current clinical practice, she focuses on treatment-resistant mood disorders and complex cases.
Dr. McInnes received Bachelor’s and Master’s degrees from Stanford University and her MD from Columbia University. She completed her residency at UCSF and research at the VA Research Fellowship and Howard Hughes Physician Research Fellowship in Psychiatric Genetics at UCSF.
Connect with forward-thinking peers, advance your practice, and attend expert events. Join the Psychiatry Collective today.
.png)

.png)
If you, or someone you know, is in crisis or needs immediate assistance, please call 911 immediately. To talk to someone now, please call the National Suicide Prevention Lifeline at 1-800-273-8255 or 988.
Osmind © 2026 All Rights Reserved.
.png)

